The Most Important Women’s Health Renaming in a Generation
In May 2026, The Lancet published the results of one of the most significant medical consensus processes in women’s health history. The conclusion: polycystic ovary syndrome — a condition affecting one in eight women globally — has been officially renamed polyendocrine metabolic ovarian syndrome, or PMOS.
For the millions of women living with this condition, and the practitioners who care for them, questions are understandably arising. Is this the same condition? Has something changed medically? Do I need a new diagnosis?
This article provides a clear, direct comparison between PMOS and PCOS — so you know exactly where you stand.
The Short Answer
PMOS and PCOS are the same condition. The biology has not changed. The symptoms have not changed. The diagnostic criteria have not changed. The treatments have not changed.
What has changed is the name — and that change was made because the old name was medically inaccurate and causing real-world harm to patients.
What Is Different Between PCOS and PMOS?
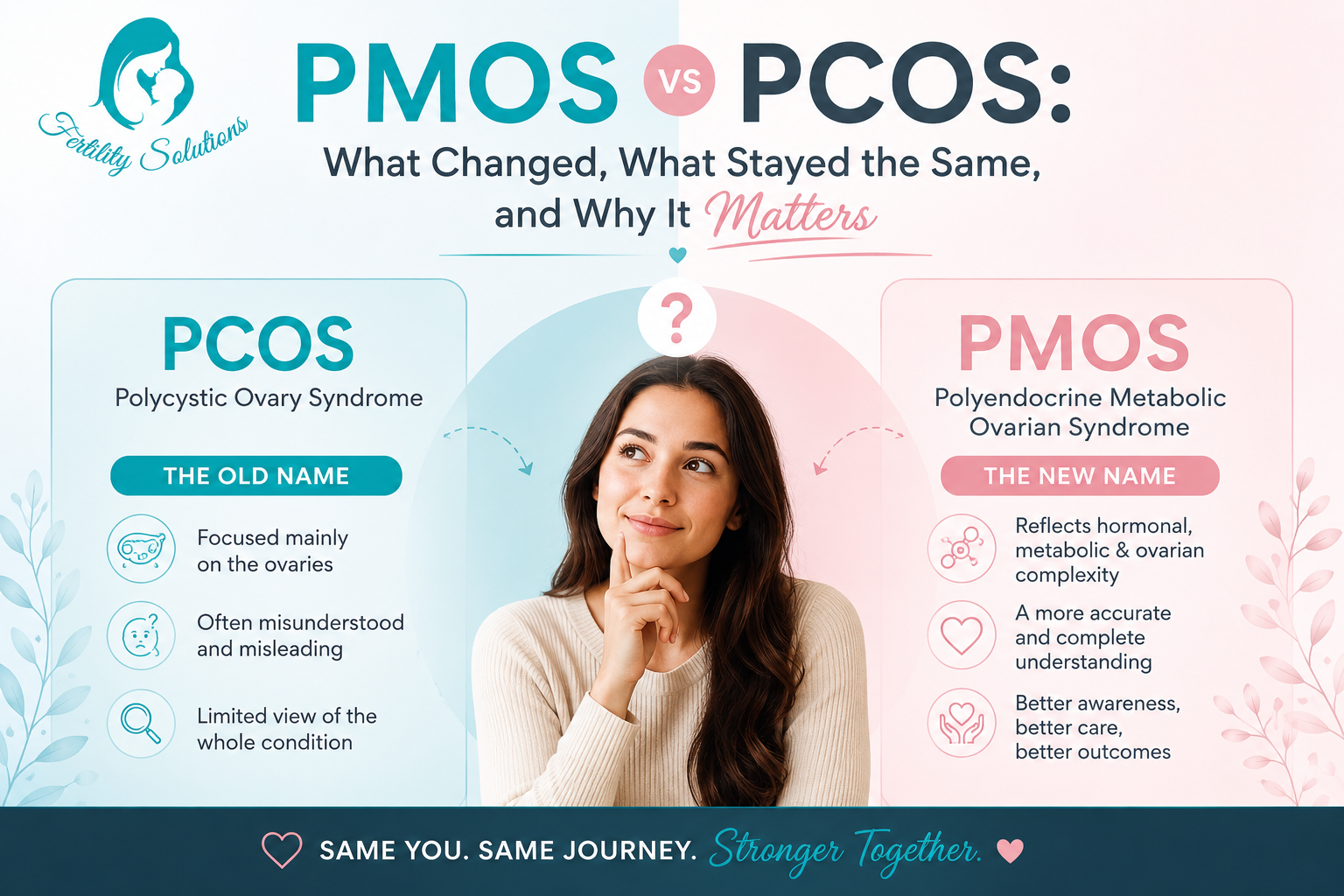
The Name
PCOS: Polycystic Ovary Syndrome — implied the defining feature was cysts on the ovaries.
PMOS: Polyendocrine Metabolic Ovarian Syndrome — reflects the condition’s true multi-system hormonal and metabolic nature.
Medical Accuracy
PCOS: Inaccurate. Women with this condition do not have pathological ovarian cysts. The name caused widespread confusion among patients and clinicians.
PMOS: Accurate. The new name captures the endocrine (hormonal), metabolic, and ovarian features of the condition without implying something that isn’t there.
Scope of Understanding
PCOS: The name framed the condition as primarily gynaecological or ovarian.
PMOS: The name communicates that this is a whole-body condition with hormonal, metabolic, reproductive, psychological, and dermatological dimensions.
Stigma
PCOS: The reproductive focus of the name caused significant distress and stigma, particularly in cultural contexts where fertility is tied to a woman’s perceived worth.
PMOS: The new name was specifically designed to reduce stigma while maintaining medical accuracy.
What Has NOT Changed?
Everything clinical about this condition remains exactly the same:
- Diagnostic criteria — unchanged. You still need to meet 2 of 3 criteria: ovulatory dysfunction, hyperandrogenism, and polycystic ovarian morphology or elevated AMH
- Symptoms — unchanged. Irregular periods, acne, excess hair, insulin resistance, fertility challenges, and metabolic features are all still part of the picture
- Treatments — unchanged. Lifestyle optimisation, metformin, ovulation induction, IUI, and IVF remain the core treatment approaches
- Your existing diagnosis — unchanged. If you were diagnosed with PCOS, that diagnosis is valid and carries forward under the PMOS framework
- The condition’s health impacts — unchanged. PMOS still carries elevated risks for type 2 diabetes, cardiovascular disease, pregnancy complications, and psychological health challenges
Why Did the Name PCOS Cause Problems?
The inaccuracy of the PCOS name had measurable, documented consequences:
Delayed diagnosis
Up to 70% of women with PCOS/PMOS are believed to have gone undiagnosed. Many women did not fit the image of ‘cysts on the ovaries’ and were either not tested or dismissed even when they met diagnostic criteria.
Knowledge gaps among clinicians
Studies showed significant knowledge gaps among doctors regarding diagnostic criteria and management of the condition — partially attributed to the name’s misleading framing.
Fragmented care
Because the old name pointed to the ovaries, many women received fertility-focused care without adequate attention to the metabolic dimensions — insulin resistance, cardiovascular risk, and long-term health management.
Research and policy misalignment
Epidemiological research, funding bodies, and policy frameworks were shaped by a name that didn’t reflect the full condition. A more accurate name is expected to improve research coherence and attract better-targeted funding.
Patient distress
Many women reported distress directly associated with the name itself — particularly around the word ‘cysts,’ which sounded alarming, and the reproductive focus, which felt stigmatising.
The Global Process Behind the Name Change
This was not a decision made by one research group or one country. The name change was the result of an unprecedented, rigorously conducted global consensus process, published in The Lancet in May 2026.
Key facts about the process:
- 14,360 survey responses from patients and health professionals
- 56 leading organisations across obstetrics, gynaecology, endocrinology, primary care, dermatology, nutrition science, and psychology
- Participants from every major world region
- Multiple rounds of Delphi surveys and in-person workshops
- Co-designed with patients, who were integral to every stage
- Marketing and cultural analysis to ensure global appropriateness
- The name PMOS was formally agreed in February 2026
The process specifically prioritised: scientific accuracy, clarity of communication, stigma avoidance, cultural appropriateness, and practical feasibility of adoption.
Why ‘Polyendocrine Metabolic Ovarian’ — And Not Something Else?
Several alternative names were considered during the consensus process. Here is why the final terms were chosen:
Polyendocrine (not just ‘endocrine’)
The prefix ‘poly’ (meaning many) was chosen to reflect the multiple hormonal systems involved — insulin, androgens, LH, FSH, AMH, and others. It also creates a familiar-sounding acronym (PMOS) that retains some continuity with PCOS, supporting an evolutionary rather than revolutionary transition.
Metabolic
Insulin resistance is present in the vast majority of women with PMOS. The metabolic features of the condition — including elevated risk for type 2 diabetes, cardiovascular disease, and metabolic syndrome — are too significant to omit from the name.
Ovarian (not ‘ovulatory’ or ‘reproductive’)
Ovulatory was considered but ultimately not chosen because it was felt to be too narrow (ovarian dysfunction involves more than just ovulation) and not applicable beyond reproductive years. ‘Reproductive’ was rejected because it was seen as potentially stigmatising. ‘Ovarian’ was chosen because it accurately encompasses the follicular, endocrine, and structural involvement of the ovaries without being reductive.
Syndrome
Retained from the original name, as it accurately describes a recognisable collection of signs and symptoms that can present differently in different individuals.
What the Transition Looks Like in Practice
A managed 3-year global transition period is now underway. Here is what to expect:
- Both PCOS and PMOS will be used during the transition — this is expected and intentional
- Your existing PCOS diagnosis carries forward under the PMOS framework
- International clinical guidelines (used in 195 countries) will be updated to PMOS terminology by 2028
- Medical records systems, disease classification codes (including ICD), and electronic health records will be progressively updated
- Patient and health professional education materials are being developed in multiple languages
- Research publications and funding bodies will begin adopting PMOS terminology
Frequently Asked Questions: PMOS vs PCOS
Is PCOS being replaced by PMOS?
Yes. PMOS is the new official name for the condition previously known as PCOS. The transition is happening globally over 3 years.
Do I need to be rediagnosed under the name PMOS?
No. Your existing PCOS diagnosis is valid and carries forward. The diagnostic criteria have not changed.
Why does my doctor still say PCOS?
The transition is gradual. During the 3-year period, both terms will be in use. Your doctor is referring to the same condition.
Is PMOS worse than PCOS, or a different condition?
Neither. PMOS is the same condition — just more accurately named. It is not a progression or a different diagnosis.
Will PCOS treatments still work for PMOS?
Yes, completely. All existing treatments — lifestyle changes, metformin, ovulation induction, IUI, IVF — remain valid and effective.
Who decided to change the name?
An international consensus process involving 56 organisations, 14,360 survey participants, and experts across obstetrics, endocrinology, reproductive medicine, primary care, and patient advocacy. The results were published in The Lancet in May 2026.
─────────────────────────────────────────────────────────────
Published by Fertility Solutions South Africa | Based on: Teede HJ et al. ‘Polyendocrine metabolic ovarian syndrome, the new name for polycystic ovary syndrome.’ The Lancet, May 12, 2026.
Disclaimer: This content is for educational purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider before making decisions about fertility treatment.
About the Author
Leigh-Ann Geydien is the founder of Fertility Solutions, South Africa’s only dedicated fertility directory. With a deep commitment to patient advocacy, she built the platform to bridge the gap between those navigating fertility challenges and the clinics and reproductive health specialists best placed to help them.