You’ve had your tests done. The results are sitting in your inbox, or your doctor has read them out over the phone. There are numbers. There are ranges. There might be the word ‘borderline’ or ‘low’ or ‘within normal limits.’ And you still don’t know what any of it means for your actual chances of having a baby.
This guide explains the most important fertility tests in plain language — what each one measures, what the ranges mean, and — most importantly — what a single number can and cannot tell you. For what happens after the results, see our guide to what your diagnosis means for your chances.
| These tests measure components of fertility, not fertility itself. A low AMH does not mean you cannot get pregnant. An elevated FSH does not mean IVF won’t work. The numbers are data points. Context is everything. |
The Tests You’re Most Likely to See
A standard fertility workup typically includes:
- AMH — Anti-Müllerian Hormone (blood test — can be done any day of your cycle)
- Day 3 FSH — Follicle-Stimulating Hormone (blood test, timed to Day 3 of your cycle)
- Day 3 Oestradiol (E2) — often run alongside FSH
- AFC — Antral Follicle Count (transvaginal ultrasound)
- LH — Luteinising Hormone (sometimes included in the Day 3 panel)
- Semen analysis — for the male partner. See our male fertility guide for a full explanation of what each parameter means.
Each one tells a different part of the story. None of them tells the whole story alone. For an overview of the complete first consultation process, see our first fertility consultation guide.
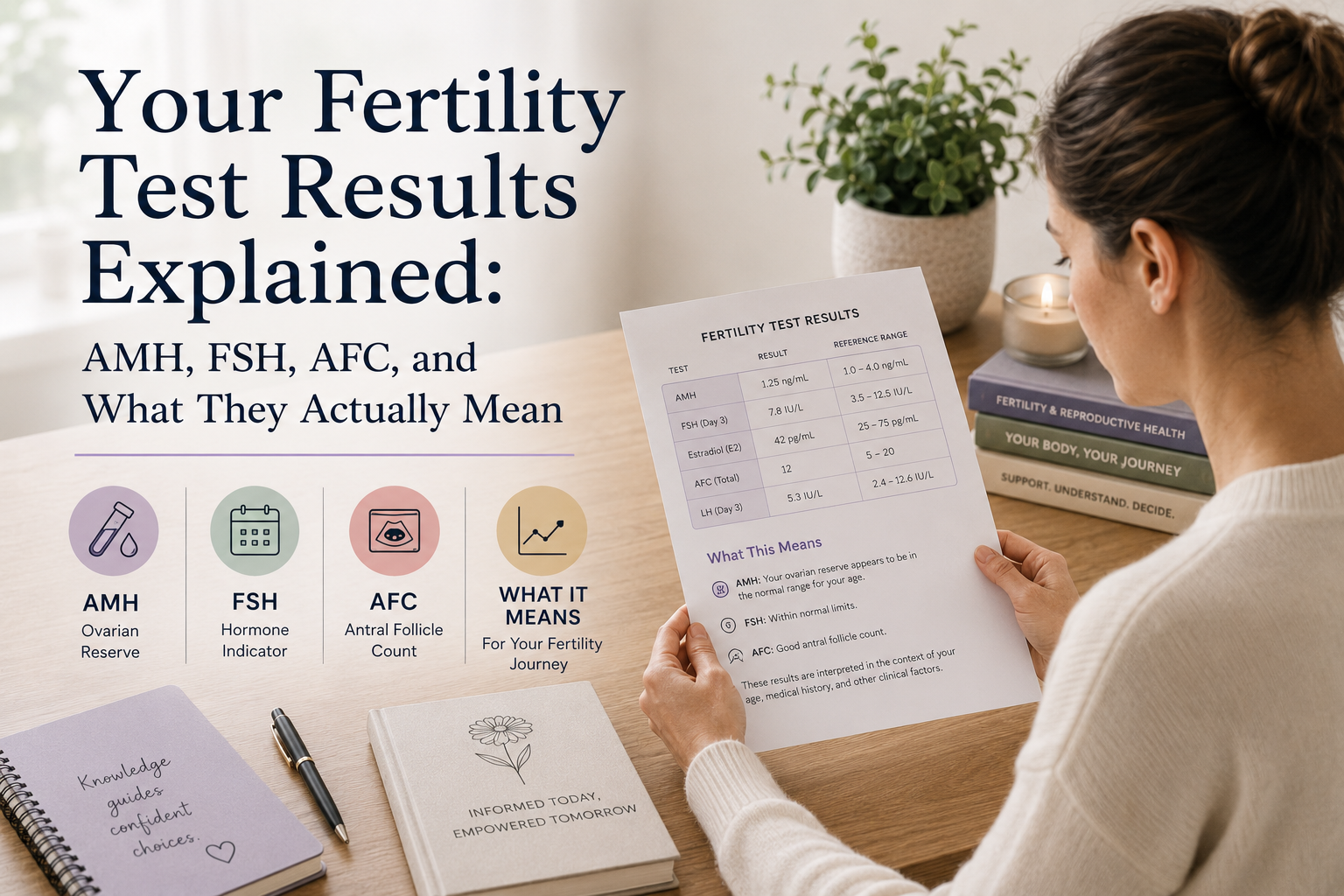
AMH — Anti-Müllerian Hormone
What it measures
AMH is a hormone produced by the small follicles (the granulosa cells surrounding developing eggs) in your ovaries. Because these follicles are constantly present regardless of where you are in your cycle, AMH is one of the most stable fertility markers — it can be measured on any day of your menstrual cycle, unlike FSH.
The level of AMH in your blood reflects the number of small follicles available — which is a proxy for your ovarian reserve — the quantity of eggs remaining.
AMH does NOT directly measure egg quality. This is an important distinction, and one that gets lost in a lot of online reading.
What the ranges mean (approximate guides — lab ranges vary)
| AMH Level | What It Suggests |
| Above 4.0 ng/mL | High reserve — may indicate PCOS; very high levels warrant investigation |
| 2.0–4.0 ng/mL | Good reserve |
| 1.0–2.0 ng/mL | Moderate reserve — typical for mid-to-late thirties |
| 0.5–1.0 ng/mL | Low-moderate — warrants a conversation with a specialist |
| Below 0.5 ng/mL | Low reserve — time is a more significant factor; specialist advice essential |
Critical caveat: These ranges are general guides only. Labs use different assays and different reference ranges. Your result must be interpreted by a specialist in the context of your age, your AFC, your FSH, and your clinical picture. A 24-year-old with AMH of 0.8 has a very different prognosis from a 41-year-old with AMH of 0.8. See our fertility by age guide for the age context.
What AMH can and cannot tell you
Can tell you: Whether your ovarian reserve appears high, normal, or reduced for your age; how your ovaries are likely to respond to fertility medication (high AMH = likely strong response; low AMH = likely lower egg yield); whether the timing of fertility assessment is more or less urgent.
Cannot tell you: Whether your eggs are chromosomally normal (quality is separate from quantity); whether you can get pregnant naturally — women with low AMH do conceive; whether IVF will work; your precise chance of pregnancy per cycle.
The most damaging misunderstanding about AMH
Low AMH = infertility. This is not accurate. AMH reflects reserve — a depleted reserve does not mean zero chance of conception. Studies have consistently shown that women with low AMH can and do conceive, both naturally and through IVF, though the margin for time is smaller and specialist input is more valuable. This is one of the most important content gaps in fertility information, and one our fertility by age guide addresses specifically.
The second common misunderstanding: high AMH is always good. Very high AMH (above 4–5 ng/mL) can indicate PCOS and may be associated with egg quality concerns. In IVF, very high AMH also increases the risk of OHSS (ovarian hyperstimulation syndrome), which affects how stimulation is managed.
| What this means for you: If your AMH came back lower than expected, take a breath before you panic. Ask your specialist what it means in the context of your full investigation — not in isolation. |
Day 3 FSH — Follicle-Stimulating Hormone
What it measures
FSH is a hormone produced by your pituitary gland that signals your ovaries to develop follicles each month. It’s measured on Day 3 of your menstrual cycle — Day 1 being the first day of full flow.
The logic: if your ovarian reserve is diminishing, your pituitary gland has to work harder to stimulate follicle development. It does this by producing more FSH. An elevated Day 3 FSH suggests your ovaries are requiring more hormonal ‘encouragement’ to respond — which in turn suggests reserve may be lower.
What the ranges mean
| Day 3 FSH Level (IU/L) | What It Suggests |
| Below 10 | Generally considered good; normal ovarian reserve indicated |
| 10–15 | Borderline — may suggest beginning reserve decline; warrants further investigation |
| Above 15 | Elevated — suggests reduced reserve; IVF response may be lower |
| Above 20–25 | Significantly elevated — reserve likely significantly reduced |
Lab ranges vary. Your fertility clinic uses specific assays and reference ranges. Always ask your specialist what their lab considers normal.
FSH vs AMH: which is better?
Both tests measure components of ovarian reserve from different angles. AMH reflects the current follicle pool more directly. FSH reflects how hard the pituitary is working to recruit follicles. Research suggests AMH is a slightly better predictor of IVF response than FSH alone (Brodin et al., Human Reproduction, 2013). However, they are complementary — a ‘reassuring’ AMH alongside a significantly elevated FSH should prompt further investigation, not reassurance.
FSH fluctuates cycle to cycle. A high result one month does not necessarily repeat the next. A single low reading does not override a pattern of elevated readings. This is why a complete picture matters — and why your first consultation should always include both markers.
Day 3 Oestradiol
This is routinely measured alongside FSH. Oestradiol (E2) at elevated levels on Day 3 can artificially suppress FSH — making FSH appear normal when it isn’t. If Day 3 oestradiol is high, the FSH result is harder to interpret. Your specialist should flag this if it applies to your results.
AFC — Antral Follicle Count
What it measures
The antral follicle count (AFC) is done via transvaginal ultrasound. The sonographer counts the small resting follicles visible in both ovaries — typically early in your menstrual cycle. These antral follicles are the ones that respond to gonadotrophin stimulation in an IVF cycle. The count is therefore a very direct predictor of how many eggs an IVF stimulation might yield.
Unlike AMH and FSH, AFC gives a visual, immediate snapshot of your current ovarian reserve.
What the ranges mean
| AFC (combined both ovaries) | What It Suggests |
| 15 or above | Good reserve; likely good IVF response |
| 8–14 | Adequate — typical for women in their mid-to-late thirties |
| 5–7 | Low-moderate — IVF yield may be limited |
| Below 5 | Low reserve; low response expected in IVF |
Important: The AFC should ideally be performed early in the cycle (Day 2–4). Later in the cycle, some follicles are further in development and the count may not accurately reflect the total resting pool.
The relationship between AFC and IVF
AFC is one of the most useful predictors of how many eggs will be retrieved in an IVF cycle. It helps your clinic decide on stimulation medication dosage and protocol. A low AFC means a lower-dose protocol won’t work — but it doesn’t mean IVF is pointless. Even with a low AFC, if the eggs retrieved are of good quality, successful outcomes are possible.
Semen Analysis: The Test That’s Just as Important (and Often an Afterthought)
Male factor infertility contributes to approximately 40–50% of fertility challenges in couples (Agarwal et al., World Journal of Men’s Health, 2021). Despite this, semen analysis is still sometimes treated as an optional or secondary test. It isn’t. It should be among the first tests done in any fertility workup. For the full guide to male fertility testing and what the results mean, see our male fertility guide.
What semen analysis measures
| Parameter | What It Reflects | Normal Range (WHO, 2021) |
| Volume | Amount of fluid per ejaculate | ≥1.4 mL |
| Concentration | Sperm per millilitre | ≥16 million/mL |
| Total count | Total sperm in the sample | ≥39 million |
| Motility (total) | % of sperm moving | ≥42% |
| Progressive motility | % moving forward | ≥30% |
| Morphology | % normally shaped (Kruger strict criteria) | ≥4% |
A note on WHO reference ranges: The 2021 WHO update revised downward the lower reference limits compared to earlier versions. A result that might have seemed borderline under old criteria may be within normal range under the updated guidelines. Confirm which criteria your lab is using.
| One semen analysis is not enough. Sperm production takes approximately 74 days, and parameters fluctuate significantly based on recent illness, stress, lifestyle, and recent abstinence before the test. A single abnormal result should typically be repeated before any firm conclusions are drawn. Most specialists recommend two results, three months apart. |
How These Tests Work Together: Reading the Whole Picture
Fertility investigations are a jigsaw, not a single photograph. Here’s how the pieces fit:
Low AMH + Low AFC + Elevated FSH: Consistently pointing to reduced ovarian reserve. This doesn’t mean pregnancy is impossible — it means time matters more and treatment planning should happen sooner. Our fertility by age guide explains the clinical implications at each age.
High AMH + Multiple follicles on scan: May indicate PCOS. The picture is not simply ‘better reserve = better fertility.’ See our PCOS and fertility guide for the specific considerations this raises.
Normal female results + Abnormal semen analysis: Male factor is the primary challenge. ICSI is likely to be part of any IVF plan. See our IUI vs IVF vs ICSI guide for how this changes the treatment approach.
Everything within normal range, still not pregnant: Unexplained infertility — one of the most frustrating diagnoses, but one with several active treatment pathways. See our unexplained infertility guide.
People Also Ask
Q: What is a good AMH level to get pregnant naturally?
A: There is no specific AMH threshold below which natural conception is impossible. Women with very low AMH (below 0.5 ng/mL) have conceived naturally. However, lower AMH generally means a smaller reserve, and seeking specialist advice sooner is prudent. The test cannot predict natural conception probability directly.
Q: Can AMH levels improve?
A: Overall ovarian reserve declines with age and cannot be reversed. However, lifestyle factors — optimised nutrition, reducing smoking, managing oxidative stress — may support the quality of existing eggs. Some studies suggest CoQ10 supplementation may have a modest benefit for egg quality. No supplement changes the underlying reserve trajectory.
Q: What does it mean if my FSH is high but AMH is normal?
A: This is a discordant result and warrants further investigation. Some studies suggest AMH may be the stronger predictor of IVF outcomes when these markers point in different directions. Your specialist should review both in the context of your AFC and full clinical picture.
Q: Is a semen analysis accurate?
A: It is a useful starting point, but it measures quantity and movement, not sperm DNA integrity — which is a separate test (DNA fragmentation analysis) that some specialists recommend in cases of unexplained infertility or recurrent miscarriage. A normal semen analysis does not guarantee there is no male factor involved.
Q: How often should I repeat fertility blood tests?
A: AMH is fairly stable and doesn’t require frequent repetition unless there is a specific clinical reason. FSH fluctuates cycle to cycle, so a single result should be interpreted cautiously. If your situation changes significantly or you’re preparing for an IVF cycle, your clinic will likely request updated tests.
Practical Takeaways
- Fertility test results are inputs, not verdicts. A single number does not determine whether you can have a baby.
- AMH reflects quantity, not quality. Low AMH does not equal infertility.
- FSH fluctuates — one cycle’s result may not reflect the whole picture. Context matters.
- AFC is most useful as an operational planning tool for IVF dosing, alongside AMH and FSH.
- Semen analysis must be part of any fertility assessment from the start — not an afterthought. See our male fertility guide.
- If your results are confusing or alarming, a first fertility consultation with a specialist is the appropriate next step — not more Googling.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Reference ranges vary between laboratories and must be interpreted by a qualified specialist.
References: Brodin T et al. (2013). AMH as a predictor of IVF outcome. Human Reproduction. | Agarwal A et al. (2021). Male factor infertility global prevalence. World Journal of Men’s Health. | WHO Laboratory Manual for the Examination and Processing of Human Semen, 6th Edition, 2021.
About the Author
Leigh-Ann Geydien is the founder of Fertility Solutions, South Africa’s only dedicated fertility directory. With a deep commitment to patient advocacy, she built the platform to bridge the gap between those navigating fertility challenges and the clinics and reproductive health specialists best placed to help them.